26.9.2012 Study Group revision - a case scenario
Today we have discussed all together with my colleagues SJ and LJ a case scenario of a 55 yoa male patient which I saw the clinic yesterday. He presented with R sided focal neck pain aggravated by rotation R>L. The patient has developed neck pain since he came back to work from the driving holiday in France one week previously. He is a smoker, drinks very little H2O, has been on BP and gout medicine for some 10 years.
The below picture shows the differential diagnosis considerations.
We concluded that each of us in their own time needs to revise what exactly is a somatic dysfunction, aneurysm symptoms, claudication and spinal stenosis, and vascular pain. The documentation that this has been revised will follow.
The below picture shows the differential diagnosis considerations.
We concluded that each of us in their own time needs to revise what exactly is a somatic dysfunction, aneurysm symptoms, claudication and spinal stenosis, and vascular pain. The documentation that this has been revised will follow.

28.9.2012 Study Group - Foot structure, function and dysfunction revision
In the study group with SJ and LJ we briefly talked through the anatomy and function of the foot. Dysfunction of the foot was discussed using mnemonics VINDICATER as seen on the picture below. We have learned that there is a difference between tarsal tunnel syndrome and tarsal sinus syndrome. We realized that we lack anatomical knowledge of the intrinsic muscles of the foot and about their function, the LEx myotomal and neurological testing and recording, and we were not sure if SLE would affect any of the peripheral joints. These topics are for a sole revision of each member of the study group. The proof of revision will follow.

4.10.2012 Study group - patient case scenarios
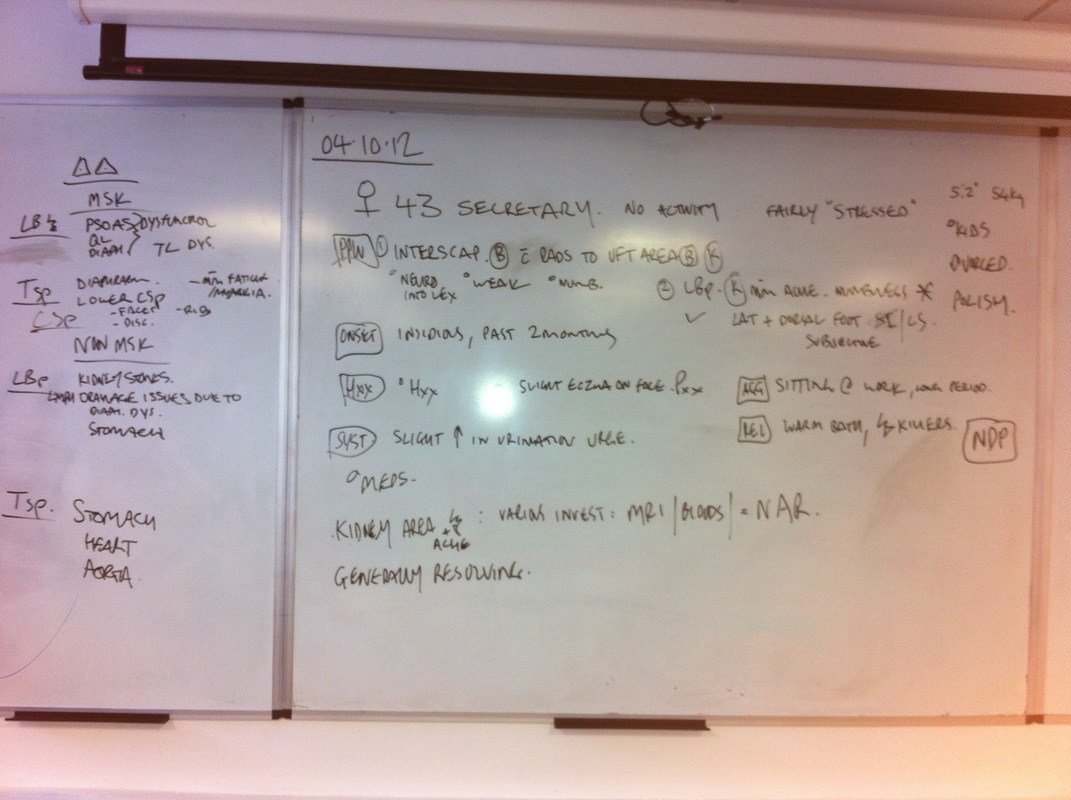
Today we talked about two cases. In the first case we discussed a patient presenting with the pain around the left shoulder blade and the upper left chest pain aggravated by deep inhalation. After scanning through all the systemic possibilities (CVS, apical tumour, PMR, pseudopseudogout), we looked at the musculoskeletal differential diagnoses. I have seen in clinic patients of this kind myself and we concluded that perhaps this presentation is quite a common one.
In the case number two LJ talked about his patient he took over from somebody else and as the patient was not getting better after eight treatments, my colleague decided to re-evaluate the patient and during this process he discovered marked structural scoliosis. Consequently we discussed the process of the scoliosis formation, how to observe and present it to the tutors. Colleague SJ talked about his experience from the summer clinic when his clinic tutor explained to him in a detail how to record the findings about the scoliosis so they are following standard medical requirements. The information should contain these points:
- is scoliosis C shaped or S shaped?
- report convexity not concavity
- state segments where the scoliosis begin and where it finishes
- at which segment is the apex of scoliosis
- is it structural or functional?
- what is the muscles state?
- what is the cob angle?
SJ was advised by his tutor to prescribe to the patients simple exercises to reverse the progression of the development of the scoliosis. We talked about types of the exercises that my colleagues prescribe for scoliosis. It was very beneficial session for me today to revise and learn some more facts about the scoliosis. Pictures below show the summaries of the two discussed cases.
In the case number two LJ talked about his patient he took over from somebody else and as the patient was not getting better after eight treatments, my colleague decided to re-evaluate the patient and during this process he discovered marked structural scoliosis. Consequently we discussed the process of the scoliosis formation, how to observe and present it to the tutors. Colleague SJ talked about his experience from the summer clinic when his clinic tutor explained to him in a detail how to record the findings about the scoliosis so they are following standard medical requirements. The information should contain these points:
- is scoliosis C shaped or S shaped?
- report convexity not concavity
- state segments where the scoliosis begin and where it finishes
- at which segment is the apex of scoliosis
- is it structural or functional?
- what is the muscles state?
- what is the cob angle?
SJ was advised by his tutor to prescribe to the patients simple exercises to reverse the progression of the development of the scoliosis. We talked about types of the exercises that my colleagues prescribe for scoliosis. It was very beneficial session for me today to revise and learn some more facts about the scoliosis. Pictures below show the summaries of the two discussed cases.

5.10.2012 Study group revision - Knee anatomy, function and dysfunction
We revised the knee today in my study group with LJ and SJ. I realised that my interest in gait and lower extremities is growing day by day. I seem to have quite a good understanding of the anatomy and dysfunction/injuries of the knee but I need to look up more on the biomechanics of the lower extremity as this seems to be so important when assessing patients with complaint of a pain while walking.... Planning to get Thomas Michaud's book on Foot orthosis as recommended by one of my tutors.

11.10.2012 Study group revision - patients case scenarios
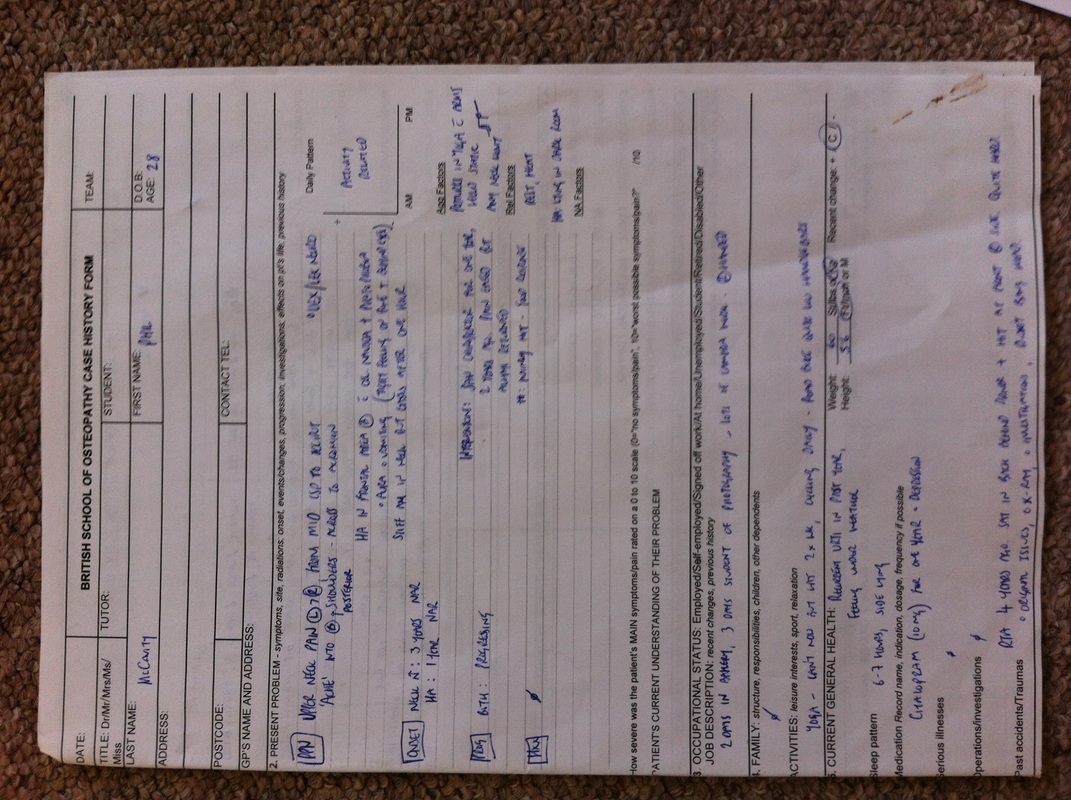
In my study group we today talked about two cases. LJ talked about his new patient clinic experience. The summary of the patient is on the picture below. Even though the patient has had no systemic problems and the knee injury seemed to be of a mechanical nature, my colleague could not provoke the symptoms on the examination. Due to the circumstances of the whole case a clinic tutor retested for the meniscal tear and his test showed positive finding. LJ was told afterwards that even the patient was in a hurry (needed to leave 20 mins earlier as the allocated time for his appointment), his examination should not have been compromised and should have been done effectively. This was a good point for all of the members in the study group to take on the board. LJ's new patient clinic tutor was D.C. who works also as an internal assessor. He grilled LJ and made him realised that knowing the detailed function of the joints of the body is necessary in order to explain the dysfunction.
My experience was from this week when I was an observing student at the new patient clinic. the case was quite complex however I could not remember all the details. Very interesting facts about the patient (detailed summary on the second picture from the top) were her L hip OA or other reason for hyper mobility and pain (severe) and L hand Raynauld's syndrome. we tried to investigate a little bit more about these problems and I came across with a hypothenar hammer syndrome causing unilateral Raynauld's syndrome in patients that practice karate or are manual workers exposed to vibrations - these damage the vessels of the hand. The patient I observed did practice karate for years however am not sure if she was left or right handed. Also the patient reported that she had a nerve block back in february this year. These nerve blocks contain steroids that apparently can cause avascular necrosis of a bone due to;
Question is: could that nerve block cause a damage to the left hip? The nerve block was injected on the left side of the spine. Interesting fact was that the patient had a multiple investigations regarding her knee OA but she was not aware of the L hip problem at all.... and she was under the physiotherapy treatment for the last 6 months.
My experience was from this week when I was an observing student at the new patient clinic. the case was quite complex however I could not remember all the details. Very interesting facts about the patient (detailed summary on the second picture from the top) were her L hip OA or other reason for hyper mobility and pain (severe) and L hand Raynauld's syndrome. we tried to investigate a little bit more about these problems and I came across with a hypothenar hammer syndrome causing unilateral Raynauld's syndrome in patients that practice karate or are manual workers exposed to vibrations - these damage the vessels of the hand. The patient I observed did practice karate for years however am not sure if she was left or right handed. Also the patient reported that she had a nerve block back in february this year. These nerve blocks contain steroids that apparently can cause avascular necrosis of a bone due to;
- either causing hyper coagulation of the blood that leads to emboli in the bone vessel, or
- alters the lipid synthesis in the liver and this can lead to fat embolism
- or this can disturb the trabeculae structure leading to collapse and necrosis of the bone.
Question is: could that nerve block cause a damage to the left hip? The nerve block was injected on the left side of the spine. Interesting fact was that the patient had a multiple investigations regarding her knee OA but she was not aware of the L hip problem at all.... and she was under the physiotherapy treatment for the last 6 months.


12.10.2012 Study group - structure, function and dysfunction of the hip joint
In my study group with LJ and SJ we revised today the hip joint. It is interesting to realise how much can one forget. We got stuck for a while on valgus and varus forces, blood supply of the hip and related problems (perthe's, SUFE). We have identified over last three weeks common problems or gaps in the knowledge we all share perhaps due to syllabus that never covered these topics or they were not sufficiently explained. these are:
can synovium swell up?
what is a blood supply of the synovium?
interrupted sympathetics to the hip - what would they cause?
how does a bone develop and grow?
PID = pelvic inflammatory disorder
snapping hip - what causes it, how to test it, what symptoms?
For the next week we have decided to revise foot, knee and hip dysfunctions and go through the orthopedic tests and techniques for treating these joints.
can synovium swell up?
what is a blood supply of the synovium?
interrupted sympathetics to the hip - what would they cause?
how does a bone develop and grow?
PID = pelvic inflammatory disorder
snapping hip - what causes it, how to test it, what symptoms?
For the next week we have decided to revise foot, knee and hip dysfunctions and go through the orthopedic tests and techniques for treating these joints.
18.10.2012 Foot problems, hip and knee testing
Today we went through the handout of NMS from the 3rd year and revised the pathology of the foot, ankle and lower leg. We talked also about the somatic dysfunction and segment facilitation. I am not sure if we came to any conclusion and the explanations vary but we felt that we have general understanding of these terms. We practiced also foot, knee and hip examination and orthopedic testing.
25.10.2012 A patient case scenario
Today we discussed the patient I saw twice and because I started the first place on thursdays, I couldnt continue to see her so my colleague and study group partner LJ is in charge of her case. Miss A has been coming to the BSO for over a year and she has not responded to the treatment so far, if anything, her upper extremity symptoms on the left side seem to be getting progressively worse. She experiences unmasking or changing neurological symptoms in her left UEx that get worse when she works. We have wrote on the board all we know about her and what testing we done and what shall we do next. We came up with possibility of a cervical rib as her symptoms strongly suggest that she suffers from TOS. However on reading on medscape we found out that TOS can effect arteries or veins only too. Thus we suggested that perhaps LJ should take a blood pressure from both her arms to see if there is any difference and also take her pulses from both arms and compare them too. The summary of the case is on the picture below.

26.10.2012 Study group - pelvis structure, function and dysfunction revision
Today we have revised pelvis following the anatomy notes from the 1st year and NMS lecture notes from the 2nd and 3rd year. We also looked at the pelvic viscera anatomy. We ended up by generating questions we would be asking the patient about their gynaecological health and also we explored the reasons for the blood in the urine.




1.11.2012 Case scenarios presentation - CCAs preparation
We have tweaked the study group sessions on thursdays a bit and this time we each prepared a case study we came across with before for our study group colleague to present to the rest of the group as in the clinic and come up with the hypothesis/differential diagnosis. We pretended to be a panel of the CCA examiners asking types of the questions we encounter in clinic. This proved to be quite a difficult task as there was a tendency of verbal description of our thought processes rather then saying which area is affected, how and what from the case history points at it. We again came across with not a clear understanding of what is a facilitated segment and what is a somatic dysfunction. For next time we decided to be more specific and we chosen 3 endocrine conditions we will implement into the case studies and will grill each other on the detail of those conditions so we are covering pathology in this way too.


8.11.2012 Case scenarios presentation with endocrine disorders involved
Today we have presented in the study group a cases that involved three endocrine disorders: diabetes type II, hyper and hypothyroidism. It was good exercise again to present to the colleagues and also be on the other side and ask the questions. next week we will be looking to do something similar on the adrenal glands and parathyroidism problems plus we are going to expand on the drugs used for these conditions.


16.11.2012 Case scenarios - Addison's, Cushing's and hyperparathyroidism
We prepared and presented to each other cases that included the presentation of the above disorders. However as they are very rare we talked mostly about steroid use in different disorders like e.g. SLE, UC or Crohn's where over the time the Cushing syndrome can be developed.


19.11.2012 Case scenarios - UC, Crohn's and IBS patients
Again very good session, we really enjoy the questioning we expose each other to and simulation of the CCA exam. I have had a case of a guy with Crohn's diseases. Important thing is to think of the kind of medication these patients are- steroids. this could cause osteoporosis and fractures. so no HVTs!


11.1.2013 Study group revision of MS, motor neuron disease and parkinson's disease.
all three of us found very helpful for our CCAs in november the presentation of the case histories with implemented disorders. we decided to carry on on fridays in the same format for couple of hours just before the technique. I had to come up with differential diagnoses for a case of a homeless man that presented with lower back pain, left medial thigh pins and needles on walking, all over stiffness, unsteadiness and that was alcoholic and currently with URTI. I found it sooo complicated. there were things I could not put together in my head and I rumbled about the abscess in the psoas area or some alcohol related damage to the neurological system. My colleagues told me that I have to stop thinking loudly and present to the tutors my ideas concisely and comprehensively. DD is this because the patient has this and that and it affects him this way. simple but difficult to do in real world. I hope next week is going to be better when we will be looking at alzheimers, cerebellar ataxia and chronic fatigue syndrome.
29.1.2013 Lumbar spine revision - NMS
today we have discussed the lumbar spine mechanics and problems that are commonly seen in the lower back. It was interesting to read through the NMS handout from the 3rd year as there were so many fact mentioned we deffinitely forgot about or they were never noticed as important. We specifically discussed spondylolysis (fracture of the pars articularis) that occurs without exception in L5 vertebra. Spondylolisthesis can be spondylolytic or non spondylolytic. the spondylolytic is due to fracture of the L5 pars articularis and the non spondylolytic is due to congenital anomaly or due to wearing off (spondyloarthosis) the facets and that one occurs mostly in L3 and L4. Spondylolisthesis can cause caude equina syndrome that is characterised by the triad of symptoms: low back pain, saddle anaesthesia and loss of sphincter control. - this is surgical emergency.
Other topic we discussed was spinal stenosis. We did not appreciate to start with how common this could be and how many different problems can cause spinal stenosis. (tumours, paget's disease, cysts, spondyloarthtritic changes etc.). Symptoms vary but cramping, pain in the back, buttocks and legs, weakness and parasthesia are common. Cervical spinal stenosis is much more dangerous as it compresses the spinal cord where else the lumbar spinal stenosis compresses cauda equina. Patients usually can cycle without discomfort (as they lean forward and this position relieves the symptoms).
Other topic we discussed was spinal stenosis. We did not appreciate to start with how common this could be and how many different problems can cause spinal stenosis. (tumours, paget's disease, cysts, spondyloarthtritic changes etc.). Symptoms vary but cramping, pain in the back, buttocks and legs, weakness and parasthesia are common. Cervical spinal stenosis is much more dangerous as it compresses the spinal cord where else the lumbar spinal stenosis compresses cauda equina. Patients usually can cycle without discomfort (as they lean forward and this position relieves the symptoms).

30.4.2013 - LJ's NP from CCA - analysis
My colleague LJ had a complicated patient with ME that he did not do well on. In the study group we analysed presenting complains the patient had. she has been vomiting in the morning, having hip pain with history of the knee and lower back pain. She complained of chest pain that came on now and then for NAR and would be hurting in sync with the heart beat. all her issues started in 2008 or shortly after. then she had first rib removed. she also had half of the stone weight fluctuation all her life.
LJ was critisised for not mentioning the possibility of the eating disorder. It did not occur to me at all during case presentation that there would be an issue with it. 3kg (half of the stone) weight fluctuation is normal in woman, before period she can store up to 2 kg of water.
My big thing was surgery and the possible effect of the removed rib and scar tissues on the vagus nerve, pleura of lungs (SOB was other thing she complained of) and on the digestion, and possible imbalance in sympathetic and parasympathetic innervation of the stomach and diaphragm (phrenic nerve also passes in the neck, so scar tissue might have influenced it). all the presenting complains were long standing and stable, so no red flags in reality.
We concluded that we would go ahead with CVS examination, respiratory examination and abdominal examination but not perhaps on the first appointment.
LJ did not consider importance of the surgery in 2008 but it is not sure if examiners would see it important and relevant either as nothing like that was mentioned in his feedback.
LJ was critisised for not mentioning the possibility of the eating disorder. It did not occur to me at all during case presentation that there would be an issue with it. 3kg (half of the stone) weight fluctuation is normal in woman, before period she can store up to 2 kg of water.
My big thing was surgery and the possible effect of the removed rib and scar tissues on the vagus nerve, pleura of lungs (SOB was other thing she complained of) and on the digestion, and possible imbalance in sympathetic and parasympathetic innervation of the stomach and diaphragm (phrenic nerve also passes in the neck, so scar tissue might have influenced it). all the presenting complains were long standing and stable, so no red flags in reality.
We concluded that we would go ahead with CVS examination, respiratory examination and abdominal examination but not perhaps on the first appointment.
LJ did not consider importance of the surgery in 2008 but it is not sure if examiners would see it important and relevant either as nothing like that was mentioned in his feedback.
30.4.2013 - SJ's patient from CCA - analysis
SJ's patient was a young woman with depression that complained of headaches and neck pain with bilateral shoulder pain. she also had dizziness and nausea and tinnitus . I was asked to analyse the case and i considered CVS and neurological issues she could have had but i did not explore in the detail all the neuro structures that influence dizziness/balance such as cerebellum, brainstem, and vestibular system. I also forgot to mention acustic neuroma for tinnitus. It was a good practice but some things got missed out.

3.5.2013 - Friday afternoon in the park revising CVS issues
It feels so amazing to be on the sun and revise for CCA. In my study group we went through CVS issues. However revision seems to be now much more relaxed, it seems that only talking about topic in a chatty was is good enough. I believe that the knowledge becomes ingrained in us to the point that we can talk about it like about weather. We have been obviously correcting and adding stuff into the conversation that made the CVS issue completely covered from anatomy, physiology, pathology and treatment point of view.
