29.11.2012 Mock CCA exam
My new patient was a 29 yoa female that presented with the lower back problem of 4 years duration with the current episode resolving. she has had a lots of falls on her back and sacrum during sporting activities. I found however her presentation a little bit confusing as she was changing the details slightly. her back pain always started in the calf of the L or R lower extremity (which one it was she couldn't recollect) where she felt cramping or pulling sensation that spread up her leg and gluteal area into the lumbar spine. I diagnosed her with L/S overstrain due to scoliosis, pelvic torsion and due to previous falls and knee injury.
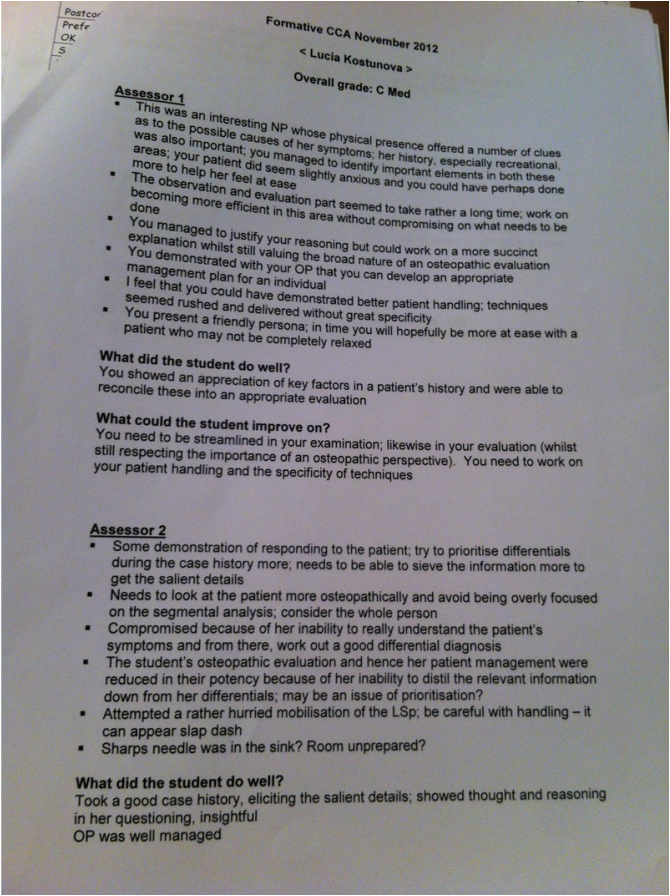
I felt time pressured and i missed some important points. I forgot to look at her from side and analyse her posture from there. neither i look at her from the front. on the neurological examination I forgot to examine joint position sense or gentle touch. I didn't check the bony levels of the pelvis from the side in order to establish which innominate was not is a correct position and what position it was. I didn't take in account the pain on palpation over sacro coccygeal joint. I gave her rushed explanation of what I found and I tried to manipulate her LSp unsuccessfully 4x!!!! I know I got Cmid from my CCA exam already however I still didn't receive the feedback so I am curious what it will have to say.
I think i need to start to write down what i am intending to do examination wise once i go back to the ttt room and have in my head an idea and an order of the thing i would do as i seem now on the regular basis to forget bits here and there and not putting things
My returning patient has presented with headaches and neck pain and also had a bunion surgery 1 year ago. I was questioned on the bunion problem a lot and what i was expected was to show ability to talk about foot while working on the neck. I can not do it!!! however I am happy that i have passed but my study group colleagues did better then me so I need to keep up good and hard work and learn from them things i have weaknesses in.
I felt time pressured and i missed some important points. I forgot to look at her from side and analyse her posture from there. neither i look at her from the front. on the neurological examination I forgot to examine joint position sense or gentle touch. I didn't check the bony levels of the pelvis from the side in order to establish which innominate was not is a correct position and what position it was. I didn't take in account the pain on palpation over sacro coccygeal joint. I gave her rushed explanation of what I found and I tried to manipulate her LSp unsuccessfully 4x!!!! I know I got Cmid from my CCA exam already however I still didn't receive the feedback so I am curious what it will have to say.
I think i need to start to write down what i am intending to do examination wise once i go back to the ttt room and have in my head an idea and an order of the thing i would do as i seem now on the regular basis to forget bits here and there and not putting things
My returning patient has presented with headaches and neck pain and also had a bunion surgery 1 year ago. I was questioned on the bunion problem a lot and what i was expected was to show ability to talk about foot while working on the neck. I can not do it!!! however I am happy that i have passed but my study group colleagues did better then me so I need to keep up good and hard work and learn from them things i have weaknesses in.

13.3.2013 CCA no.1
I was very nervous before the CCA exam but as soon as I started to talk to my first patient i took it as a normal thing. My first patient came in with chronic duration of right wrist pain that I diagnosed as RSI of extensor carpi ulnaris muscle. I examined her wrist and elbow but did not think it would be necessary to ask her to undress in that stressful situation. While presenting the findings of the examination to the examiner I explained that i noticed on the elbow examination that there is a limited external rotation of the right shoulder and I explained i would like to investigate it on the next appointment. He questioned me why i did not do it then and there. Oh well, i just panicked! I could not explain RSI pathophysiology either.
My second patient was a lady with multiple biopsychosocial issues and systemic symptoms. I came up with multiple possibilities and need to refer her for some further investigations regarding her issues, however non of them were red flag. her complain was a neck pain. O overrun quite a lot but it was ok as her case was quite complex and i received positive feedback on this.
My returning patient however did not go that well. I think i might chosen a patient that was too complex and I could not include everything on one A4 sheet of paper. She has been my patient for over 1 and 3/4 of the year and has had flare up of different problems that in the mean while resolved however I treated her for general mild degenerative changes in her lumbar spine and neck and addaptation of the body to dropped medial arch of the right foot. What made the whole situation completely awkward was the noise coming from the street - some road works due to which i could not hear my examiner asking me questions, my patient was completely nervous and i could feel it.... they left me with her after 5 minutes as there was no point to carry on questioning me on anything in this sort of conditions. I did not even get a proper feedback on my returning patient... well, I passed so not too bad. Below is the copy of the examiners feedback.
My second patient was a lady with multiple biopsychosocial issues and systemic symptoms. I came up with multiple possibilities and need to refer her for some further investigations regarding her issues, however non of them were red flag. her complain was a neck pain. O overrun quite a lot but it was ok as her case was quite complex and i received positive feedback on this.
My returning patient however did not go that well. I think i might chosen a patient that was too complex and I could not include everything on one A4 sheet of paper. She has been my patient for over 1 and 3/4 of the year and has had flare up of different problems that in the mean while resolved however I treated her for general mild degenerative changes in her lumbar spine and neck and addaptation of the body to dropped medial arch of the right foot. What made the whole situation completely awkward was the noise coming from the street - some road works due to which i could not hear my examiner asking me questions, my patient was completely nervous and i could feel it.... they left me with her after 5 minutes as there was no point to carry on questioning me on anything in this sort of conditions. I did not even get a proper feedback on my returning patient... well, I passed so not too bad. Below is the copy of the examiners feedback.


